

Got back pain?
This is a study that compares two different treatment approaches head to head. Bout damn time that we are looking at two approaches and comparing them in a study. We (health care researchers) typically compare one treatment against no treatment. This is good and all, but then we believe that all treatments work and work equally. These are the types of studies that need to come out, so that as a health care provider, I am providing the best treatment to help your problem.
- “A recent UK survey estimated the (1-month period) prevalence of spinal pain to be 29%”
This means that during any one month period about 1 in 3.5 people are experiencing back pain, over on the other side of the pond. Think about that! If you have one person on each side of you, one of you will have back pain during the month.
- “The lifetime prevalence of these conditions is also high—it is estimated that »70-85% of the population will experience some spinal pain during their lifetime”
Again, 8 out of 10 people will have back pain during their lifetime. This is starting to sound grim. Pain is not normal. What are we doing to ourselves? Why do we keep having back pain at such an alarming rate? I have my opinions, based on some research, but it hasn’t been fully substantiated yet. I will pull out the research at a later date of course.
- “In 1998, the cost of lower back pain alone to the UK National Health Service was estimated at 1 billion (pounds), with over 200 million (pounds) being spent on physiotherapy”
So…what’s this got to do with us? That’s the UK. The numbers aren’t too far off of what we are spending on back pain. See the link from a previous post in which I discuss monetary figures.
https://movementthinker.org/2016/03/17/a-little-bit-of-crazy/
- “guidelines state that in the first instance patients should be encouraged to remain active, with the prescription of anti-inflammatory drug and/or analgesia where required.”
There is an opiod epidemic spreading world wide. I realize that opiods and anti-inflammatories are a long ways away from each other, but to think that back pain will be fixed with medication only is dreaming. NSAID’s are not always the answer either. http://www.aafp.org/afp/2002/0401/p1319.html
Robin Mckenzie states in his textbook (paraphrased): a mechanical problem needs a mechanical answer and a chemical problem needs a chemical solution. The first question has to be: is the pain mechanical or chemical?
To remain active is the same advice that I could get from my dad. You’ve heard the advice countless times I’m sure…especially if you’ve ever been hit by the ball while standing in the batter’s box…”walk it off”. Hell, my dad was a laborer. He didn’t go to medical school, but gives the same advice. I pay for better than that. I can get the advice for free back in Elwood.
- “Physiotherapy treatments aimed at alleviating the physical causes of back and neck pain include: advice, exercise programmes, massage, mobilization and manipulation”
Some big takeaways from this sentence are what was left out of the sentence. At no point did the authors talk about ULTRASOUND!, ELECTRICAL STIMULATION!, TRACTION!, VAX-D (sp)! CUPPING! or any of the other passive fads that make clinics money for doing thoughtless work. Look…if the above (in capital letters) makes up a part of your treatment, you have to question your practitioner as to why and what are the expectations of the intervention. I know what my expectations are…lining the owners pocket with greenbacks.
- “a new type of intervention for treating back and neck pain has recently been developed, triggered by growing awareness that psychosocial factors play an important role in musculoskeletal complaints. These behavioural interventions have different compositions depending on the specific theory underpinning the approach.”
To think that the “biopsychosocial” approach is new is a fallacy. It is a newer concept to put a name to it, but even those that simply have “mechanical” training understand that in order to use “mechanical” training, we have to get through the psychosocial constructs of each patient.
- “elucidating whether a treatment offers good value for money in terms of cost vs benefit must also be considered”
This is an interesting topic that is finally coming to the forefront in healthcare. I’m going to go to the extremes to make a point. Let’s say that you have a heart problem and a surgery that costs 100,000$ will keep you alive for decades, but a surgery that only costs $1,000 can keep you alive for a year. Which would you take? Costs vs benefits become very apparent in this scenario. This article will scale the topic down to back pain.
- “The trial compared two physiotherapists delivered interventions for musculoskeletal back and neck pain, which aimed to promote return to normal activities…Solution Finding Approach, was a brief physiotherapy intervention based on cognitive behavioral principles…a patient-centred view and, in this context, aims to help patients identify reasons for their pain and to provide solutions and long-term management strategies”
This essentially says: this approach consists of few physical therapy visits in order to help you figure out why you have pain and to provide solutions to long term management of your pain.
Remember this because it is important for the next section.
- “The second approach was the more traditional biomechanical approach used by physiotherapists, the McKenzie approach, which involves classification of patient’s spinal condition and the prescription of specific therapeutic exercises.”
This one states the following: The therapist will help you figure out why you have pain, through a classification system, and issue solutions (exercises) in order to provide long term management of your pain.
Sounds fishy…I don’t know if I like either method since they both sound so similar. Those that know me, know that I am biased. I am certified in the McKenzie method, formally known as Mechanical Diagnosis and Therapy.
- MeKenzie approach…has been clearly documented…commonly used by physiotherapists…conducted a biomechanical assessment using repeated movements of the spine and, based on these findings, prescribed specific exercises for the patients to work on repeatedly themselves…relies on active compliance with the exercises and advice.”
MDT (McKenzie method) was created a long time ago. I know the history like the back of my hand, but it seems like too much to type out here. Look up his biography, “Against the Tide” to read how this man revolutionized the way spines and now extremities are treated…by those that have studied the method. In a time in which not many believed him, and many went so far as to ridicule his methods, it took almost 50 years to confirm his thoughts through science.
Anyway, we use repeated, sustained, resisted and speed based positioning in order to elicit a change in symptoms. Manual techniques can also be used to elicit a change. Once we see a change that is documented with having good results…we stop there and send you home with the exercise, position or movement.
- “All the physiotherapists delivering the McKenzie approach were experienced in this method and had undertaken McKenzie Institute training (courses A-D).”
This is important. Scott Herbowy, one of the highly trained professors of the method, published a study in the recent years regarding the training and outcomes of those using the methods. It seems realistic to believe that someone that has taken courses A-D would have the same reliability and outcomes as someone that has taken the same courses and passed a competency exam. This is not true though. Those that have not yet passed the test appear to be inconsistent in classifying patients using MDt. See the study below to learn more:
http://www.ncbi.nlm.nih.gov/pubmed/24253786
- “…both the McKenize and Solution Finding approaches lead to improvements in patient outcomes over time, with no significant differences between the two treatments.”
Both treatment ideas provide similar improvements over time. This indicates that just in terms of improvements, it doesn’t matter which method is used (albeit neither group of therapists were highly trained in using the intervention attempting to be studies). I liken this to asking an auto mechanic to work on a Boing Jumbo Jet. Yes…the mechanic understands engines, but there’s a difference in specialties.
- “The McKenzie treatment required on average, one extra subsequent visit to the physiotherapist”
This means that seeing a therapist semi-trained in MDT will cost you an extra $100 dollars compared to seeing someone semi-trained in the Solution Finding Approach. Is this a bad thing? We will see.
- “the Solution Finding Approach is slightly cheaper than the McKenzie approach but confers marginally lower benefit”
Dave Ramsey has a free radio show about finances. One of his taglines is “the advice is worth what you pay for.” Obviously he’s kidding, but we all know that the better stuff in life isn’t free. When it comes to your health, how much more are you willing to pay? Are you willing to pay “slightly” more?
- “The policy maker needs to decide whether she or he is willing to invest additional health care resources funding the McKenzie approach”
Look, you need to find someone that has this certification or diploma training if you have back pain. Countries are debating whether or not more money should be put into training therapists in this method. Some of us have paid for the training out of pocket in order to become better therapists, with the end goal of providing great care to patients.
- “the additional cost associated with the McKenzie treatment is worth paying, given the additional benefit it provides”
NEED I EXPAND ON THIS SENTENCE? This benefit is from people that aren’t even “minimally competent” to provide this service. Imagine how much more benefit or less cost that you would have from someone that is competent in using the method.
This study was performed in the UK. There is no reason for me to believe that back pain differs that significantly from those experiencing back pain in the US. I have to correlate that those seeing a McKenzie Credentialled therapist will see even better results or spend less money over the long haul than that those seeing someone using cognitive behavioral therapy.
Quotes taken from: Manca A, Dumville JC, Torgerson DJ, Moffett JAK, et al. Randomized trial of two physiotherapy interventions for primary care back and neck pain patients: cost-effectiveness analysis. Rheumatology 2007;46:1495-1501.
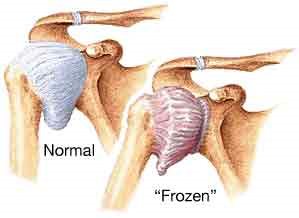 Frozen shoulder, when it doesn’t move.
Frozen shoulder, when it doesn’t move.