
- Lumbar spinal stenois (LSS)…defined by any narrowing of the spinal canal and/or nerve root canals…In patients with severe LSS, a space reduction of 67% has been found in the spinal canal.”
Spinal stenosis is the narrowing of the holes of the spine. The spine has 3 holes in it in the lumbar region. Each hole carries a nerve. It could either be the nerve of the spinal cord down the middle, and larger, hole. It could be the nerve roots out of the holes on the side of the spine. Each hole needs to be big enough so that it doesn’t irritate the nerve that it allows to pass through the hole. Picture a water pipe. If you put too much stuff in the pipe it will clog up. Sometimes there are tissues that can make their way into the holes of the spine to clog the holes. When the hole is clogged, the nerves don’t have as much room to do their job (transmitting signals to and from the brain). Now take that same pipe and come back and look at it over decades. There will be sludge and stuff built up around the pipe. This is essentially creating a smaller diameter on the inside of the pipe. This smaller diameter due to sludge is also creating a smaller hole. This could happen in the spine with severe arthritis or degenerative disc issues in which the hole gets smaller. A visual is much better so maybe this will help. image for spinal stenosis
- “…estimated the incidence of LSS in Denmark to 272 per one million inhabitants per year”
In other words, it is not very common in Denmark.
- “…it is important to discriminate between LSS and disc generated pain since these conditions have different prognoses and the range of evidence based treatments are different, as well.”
The treatment between the two issues, discogenic back pain and stenotic back pain, is very different. A thorough evaluation can start to correlate symptoms with either discogenic pain or non-discogenic pain. Many patients believe that an MRI will be the answer to why they have pain, but unfortunately this isn’t so.
- “a valid and reliable clinical assessment protocol for identifying LSS would be valuable in terms of choosing relevant treatment and informing the patient about the prognosis as early as possible.”
This article was written in 2009. The medical profession has existed for eons. There is still not a valid way to assess a patient in order to determine spinal stenosis. There are biologically plausible ways, meaning that when I assess you, I can make an educated guess from some of the findings in the history and physical, but it is not a valid (proven) way of coming to a conclusion.
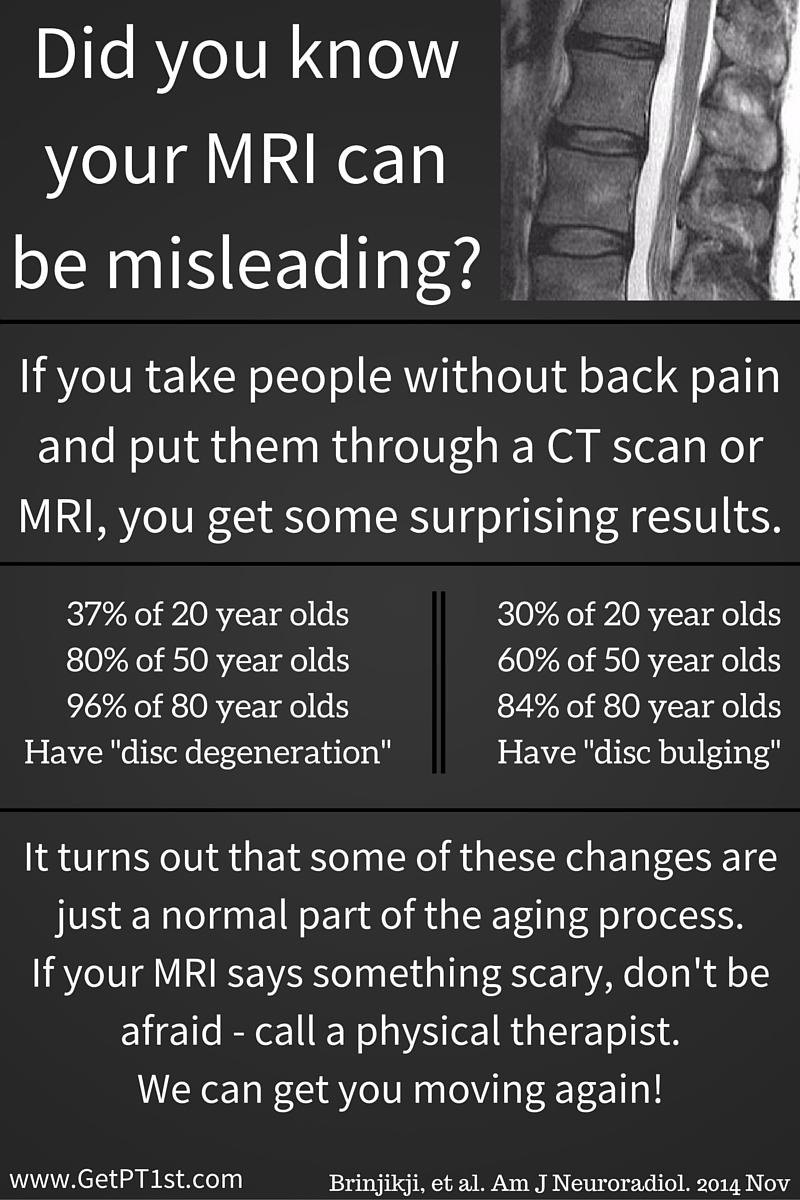
- “The high sensitivity and specificity of MRI suggests this is a good test for ruling in and out the disease.”
The MRI does a great job of telling us what is abnormal, but it doesn’t do a great job of telling us if the abnormal finding is causing symptoms. As seen in the link above, there are abnormal findings in a population without symptoms. We have to take the imaging findings and see if they make sense after performing a physical exam.
- “…history will provide strong clues to the presence of spinal stenosis…more than 65 years of age…prolonged history of low back pain and intermittent radiating symptoms having developed gradually…limited walking capacity…Movements or positions involving flexion e.g. sitting or stooping, will often abolish symptoms…total loss of lumbar extension range is usually found, while flexion most often is well preserved.”
The typical patient with lumbar spinal stenosis will notice that the ability to walk has gradually reduced over time and there is a need to sit due to back or leg pain. Sitting will typically turn down or off the symptoms rapidly. This patient will have limited motion into extension (think of looking over your head to see the stars or bending backwards while standing).
- “…stenosis from zygapophyseal joint hypertrophy, ligament thickening or other degenerative changes, it cannot be expected that physical exercise or manual treatment will create a lasting change in the degree of space reduction in the spinal canal or intervertebral foramina”
In the presence of physical changes to the bones, ligaments or loss of disc height, there is nothing that a PT can do to change these back to the way that they were previously. These have been described as wrinkles on the inside. If we look at your face we can start to see how much age you have based on the wrinkles in the face. This is also done on the inside in that some “degenerative” changes are normal. Wrinkles are normal; they are not symptoms of anything sinister. The same can be said for physical changes on the inside. They don’t have to be pain generators. It takes a physical exam to determine how your symptoms respond and whether or not this matches the images on an MRI or X-ray. Even then, we can’t say that movement won’t help, only that we won’t change the physical “inside wrinkles”.
- “The main purpose of this pilot study is to evaluate the validity and intertester reliability of an algorithm of physical examination tests, in relation to identifying symptomatic lumbar spinal stenosis.”
This is good. A pilot study is like a pilot for a t.v. show. This is done to see if additional episodes should be done. This study will conclude if additional studies on this topic should be done. What it hopes to find is a reliable (consistent) way of determining validity (actually seeing what the test hopes to see) in testing for lumbar spinal stenosis. A test that is both reliable and valid should be able to test for spinal stenosis regardless of who is performing the test and who is measuring the test.
- “Two patients were classified as “LSS” and five patients “Not LSS”, meaning a 29% prevalence of “LSS” Intertester agreement for overall diagnostic conclusion was 100%”
There are so few patients that this study will likely not yield any results that are actionable. The interesting thing is that the examiners agreed 100% of the time. This is not common in the medical field to have 100% agreement on near anything.
- “…the algorithm in its present form can not be used as a screening test to rule out LSS, although it may be able to diagnose the condition.”
There were so few people in the study that it is hard for any clinician to put it to use in the clinic. It may be able to diagnose the condition in that it demonstrated a specificity of 1.0, which is really good.
Excerpts taken from:
Lengsoe L, Lyhne S, Melbye M. An algorithm for clinical identification of spinal stenosis-a pilot study of validity and intertester reliability. International J of MDT. 2009;4(2):21-28.
Can’t find the abstract to the study, but it is listed under the author’s CV http://pure.au.dk/portal/en/persons/martin-melbye(ed4ee688-2d9e-4c17-b0b1-44a5b4b59ada)/publications/an-algorithm-for-clinical-identification-of-spinal-stenosis–a-pilot-study-of-validity-and-intertester-reliability(6d714ee0-d910-11de-9e3b-000ea68e967b).html
 You are not your MRI…at least not for long.
You are not your MRI…at least not for long.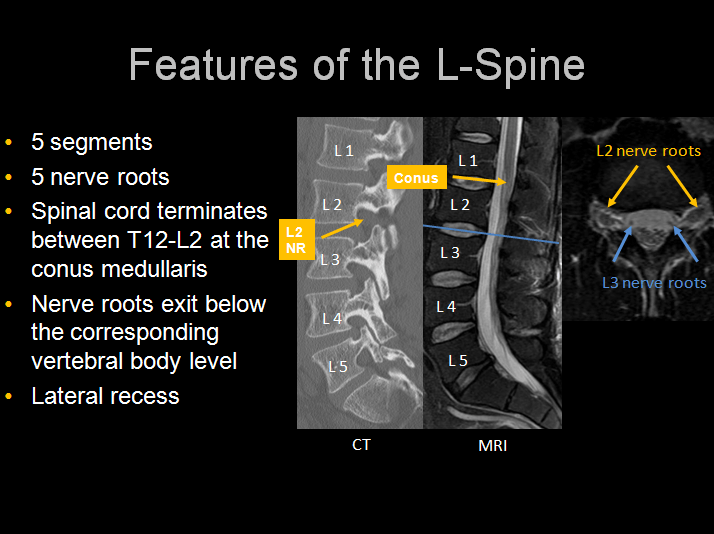
 SCIATICA OF THE ARM
SCIATICA OF THE ARM
{kind=link}