 Frozen shoulder, when it doesn’t move.
Frozen shoulder, when it doesn’t move.
Frozen shoulder is a common diagnosis in the clinic. I have seen this problem treated in so many different ways that some PT’s are able to drive Escalades. The problem is that not all treatments are created equal. Educate yourself on what the problem is and how it can and should be treated. It’s your body…understand it at least.
- “Frozen shoulder, or adhesive capsulitis…painful and limited active and passive range of motion…reported to affect 2% to 5% of the general population”
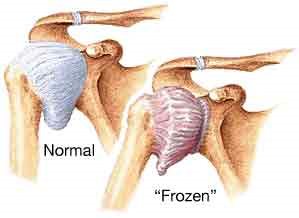
To be frank, frozen shoulder means your shoulder is frozen…it doesn’t move. Adhesive capsulitis is the medical term for…your shoulder doesn’t move! If you take something that does’t move and you try to move it…it is painful. It is not as common as everyone would like to believe and honestly I rarely see it in the clinic. You can have a stiff shoulder and not necessarily have “frozen” shoulder. It affects those that are diabetic more often than those that aren’t, but aside from this, the reason for it is still not certain.
- “The absence of standardized nomenclature for frozen shoulder causes confusion in the literature”
We know some things for certain. Your frozen shoulder will go through stages from start to end, what we aren’t certain of is how many stages, and what do we call these stages?
- “Secondary frozen shoulder was defined by 3 subcategories: systemic, extrinsic, and intrinsic…secondary frozen shoulder related to insulin-dependent diabetes are more likely to have a more protracted and difficult clinical course”
If you have frozen shoulder because of some other problems, this is classified as secondary. If that problem is due to a body disease, extrinsic is due to an injury outside of the shoulder and intrinsic is a known problem of the shoulder.
- “another classification system based on the patient’s irritability level (low, moderate and high) that we (the authors of the journal article) believe is helpful when making clinical decisions regarding rehabilitation intervention…Patients with low irritability have less pain and have capsular end feels with little or no pain; therefore, active and passive motion are equal and disability lower…typically report stiffness rather than pain as a chief complaint…high irritability have significant pain resulting in limited passive motion (due to muscle guarding) and greater disability…pain rather than stiffness…”
This is very easy to follow…walk with me. Your irritability is literally that, when you move how irritating is it? If it is not that painful and you have a capsular end-feel (only to be determined by someone that has moved thousands and thousands of shoulders so that it can be determined if the joint is normal or not very moveable), then it is lower on the scale of irritable. If your shoulder feels like a hot poker stabbing you in the eye and twisted every time you move the shoulder…it’s probably highly irritable.
- “recent evidence identifies elevated serum cytokine levels as part of the process. Cytokines and other growth factors facilitate tissue repair and remodeling as part of the inflammatory process…sustained inflammation and fibrosis…although the initial stimulus is unknown.”
This is HUGE, for those that are nerdy regarding physiology. Tendonitis…doesn’t exist. That’s a lie, but not far off. When you think that you have a tendonitis, by the time you see a doctor, it is probably a tendinosis. This means that after a short period of time, there are no longer inflammatory markers (chemical of inflammation) in the tendon. The fact that there is sustained inflammation is…NO GOOD! Think about having constant cycles of inflammation going on in your body. It sounds painful. It is! Others have challenged the premise of adhesive capsulitis, in that the capsule itself doesn’t have the inflammatory markers. At this time, it is semantics, because the shoulder is still painful.
- “3 sequential stages: the painful stage, the stiff stage and the recovery stage” others have described “4 stages…the preadhesive stage, the acute adhesive or freezing stage…the fibrotic or frozen stage…the thawing phase” these phases may take 12-18 months and “mild symptoms may persist for years”
Although we can’t fully agree on how many stages and how to describe the stages, we know that this is will take a long time in order to become fully functional.
- “A full upper-quarter examination is performed to rule out cervical spine and neurological pathologies”
I can’t stress this enough. Just because your shoulder hurts, doesn’t mean that your shoulder is the problem. I refer to the spine as the great chameleon. It can mimic damn near any symptom that you experience in the periphery. If you don’t fully evaluate the spine…or at least take a quick peek…then you may be treating the wrong thing!
- “typically reveals significant limitation of both active and passive elevation, usually less than 120 degrees”
Quick lesson, active elevation is your ability to raise your own arm. Passive elevation is your ability to allow me to raise your arm. Those with rotator cuff tears or issues typically have horrible active elevation, but passive elevation is much better and may be normal.
- “Scapular substitution frequently accompanies active shoulder motion…” and “Cyriax described a capsular pattern he believed diagnostic for adhesive capsulitis…it is not consistently seen in patients with frozen shoulder when objectively measured.”
Scapular substituion is elevating the shoulder blade in order to perceive that your are raising your arm further overhead. I tell patients to look at the space between your shoulder and your ear. If there is a huge change in that space when raising your arm overhead, then something is wrong. Patient’s will understand this visual. Have them do it with their “healthy” side so that they can see how much space change actually occurs and then do it with the problematic side to compare.
Cyriax, think Alfred Hitchcock look-alike, is one of the greats that provided many thoughts in the infancy of our profession. His theories are still taught in school and we still have to memorize his paradigms for examinations. In real practice though, we don’t always follow his teachings because…they aren’t always right. Each therapist will learn through seeing thousands and thousands of shoulders, that his patterns aren’t always right, but aren’t always wrong.
- “Although authors of textbooks have described patients with frozen shoulder as having normal strength and painless resisted motions…revealed significant weakness of the shoulder internal rotators and elevators.”
In school we learned that frozen shoulder doesn’t affect strength. I am not sure if it is still being taught, but I have to believe so because the boards (think OWL exams from Harry Potter) are based on the text books and not on recent research. Regardless, theses patients do demonstrate weakness. In my opinion, this weakness may be related to disuse due to pain or pain inhibition, but that is a story for another day.
- “Significant loss of passive external rotation with the arm at the side, as well as loss of active and passive motion in other planes of movement, differentiates frozen shoulder from other pathologies…Early frozen shoulder may be difficult to differentiate from rotator cuff tendinopathy because motion may be minimally restricted and strength testing may be normal”
Big picture…frozen shoulder will present with multiple losses of motion in many planes. Early frozen shoulder will still have ROM limitations, but not as bad as those that are in the second stage, which may make it difficult to see at first. The therapist/MD may not immediately recognize frozen shoulder and the treatment may be inconsistent with what is needed.
- “The definitive treatment for frozen shoulder remains unclear…Establishing treatment effectiveness is also difficult because the majority of patients with frozen shoulder significantly improve in approximately 1 year; therefore, natural history must be considered”
In other words, we think we know how to treat it, but even if we don’t you will get better over time. Is it possible that you don’t need to come to therapy…of course! Will you benefit from therapy…of course! Even if the therapist is providing stuff that doesn’t work…like ultrasound…the therapist should be spending adequate time with you in order to educate you regarding the condition and the overall prognosis. If your health care provider is not doing this…walk away! There are therapists on almost every corner if you look hard enough. Find one of quality.
- “Explaining the insidious nature of frozen shoulder allays the patient’s fear of more serious diseases…prepares the patient for an extended recovery…because daily exercise is effective in relieving symptoms”
This is my primary job…education. I gave up a career, as a teacher because I felt the system was broken. It is too hard to teach a group of kids when I had to cater to lowest common denominators. In this profession, I am still a teacher, but I only have one student…the patient in front of me. If I can teach you everything you need to know in one visit and you will go out and be the perfect patient, I may never have to see you again…for this at least. Most patient’s can’t absorb everything and may not be overly compliant after the first visit, so more visits will be needed. My hope is that the frequency of our meetings will decrease over time as the patient takes more ownership over lifestyle changes and exercise performance. Alas…sometimes it never happens.
- “Little data exist supporting the use of frequently employed modalities such as heat, ice, ultrasound, or electrical stimulation.”
If this comprises a majority of your therapy…”Houston, we have a problem”. I’ve said it before and I’ll continue to stand on the soap box. Health care is a business. All businesses need to keep the doors open and it would be nice if there was a profit at the end of the day. This means that you will be charged for unsupported treatments because of the following reasons: 1. Patients expect this, as this has traditionally been sold as physical therapy 2. It feels good 3. It pays well.
- “Gursel et al demonstrated the lack of efficacy of ultrasound, as compared to sham ultrasound, in treating shoulder soft tissue disorders”
It is no better than a placebo! If you would pay for it out of pocket, then I would rub some lotion over you with an ultrasound and then tell you that it is not effective. Would you still pay for it? If the insurance covers it though…why not? I will tell you why not…it takes up valuable time that I could be focusing on something more effective.
- “The basic strategy in treating structural stiffness is to apply appropriate tissue stress…think of the total amount of stress being applied as the ‘dosage’, in much the same way that dosage applies to medication…adjusting the dose of tissue stress results in the desired therapeutic change”
Tissue stress is anything that stresses the tissue. I know that it sounds simple…DUH. It is. I can stress the tissue by squeezing the tissue, stretching the tissue, forcing the tissue to contract against an outside force, but in the end, I need to provide the “appropriate tissue stress”. If the tissue is shortened, then it needs to be lengthened. This occurs by stressing with stretching. You will have to follow a prescribed set and repetition scheme at a specific interval frequency, which will be given by your therapist. Typically this is performed no earlier than every 12 minutes and no later than every 3 hours.
- “Three factors should be considered when calculating the dose…intensity, frequency and duration.”
Think of these as variables. Any good scientist knows that the best way to find the variable most important is to only change one variable at a time. If the patient presents to therapy and is not making progress, then I can change any of the three variables. I will choose to change the variable that 1. Best fits with the patient’s schedule 2. Gives me the lowest chance of making the patient worst 3. Gives me the predicted best result. All in this order. If I give you an exercise that you can’t do, then it doesn’t matter if I believe that it will help you. For instance, if I give you an exercise that needs to be done lying, but you work in a sewer system, you may not like me after the exercise.
- “Aggressive stretching beyond the pain threshold resulted in inferior outcomes in patients…tissue stress is progressed primarily by increasing stretch frequency and duration”
Going to therapy 3 days per week and expecting the therapist to get you better is a pipe dream. If you only go to the therapist for stretching, then the intensity will be high. This will result in an inflammatory effect, in which you will not want to/be able to move your shoulder. At this point, the stiffness will worsen. Be smart and move to tolerance. If you are worse for more than 20 minutes after stopping, you made a mistake and went too intense (there is research to support this timeline, but I don’t have it onhand).
- “Patients with the worst perceptions of their shoulder before treatment tended to have the worst outcomes.”
Butterflies and rainbows. If you think you are disabled, then you are. Please move. PSA.
- “Many authors and clinicians advocate joint mobilization for pain reduction and improved ROM. Unfortunately, little scientific evidence exists to demonstrate the efficacy of joint mobilization over other forms of treatment for frozen shoulder.”
I can easily spend 20 minutes mobilizing your shoulder and small talking about the weather, politics and religion. How else are we going to talk for 20 minutes?! That’s a long time for me to hold your arm. I need something to pass the time. The evidence is conflicting regarding me pressing on your shoulder to try to free up some room. I do mobilizations sparingly. They are good to know and if nothing else is working, then sure…why not do them? If something else works better, then that’s why I don’t do them often.
- “improved extensibility of any portion of the CLC (joint capsule) results in improved motion in all planes.”
I love using this example in the clinic: There was an episode of Seinfeld in which George and Jerry were staying in a fancy hotel. George went on this rant regarding tuck vs no tuck. Big picture…when the sheet is tucked in too tight, it is impossible to move your feet. You have to loosen up the sheets by kicking at them. Once you’ve loosened it up a little, it seems to free up a ton of room everywhere. This is the circle concept of the shoulder.
When we loosen up on aspect of the capsule, then the laxity that is created just moves around the capsule through additional mobilizations. We don’t actually stretch out the capsule in multiple planes.
- “At 7 weeks, 77% of the patients treated with injections were considered treatment successes, compared to only 46% treated with physiotherapy.”
Hell, this stat makes me want to advise patients to do this first before seeing me…or start gambling for the night. Does anyone else see the 777?
- “The core exercises include pendulum exercise, passive supine forward elevation, passive external rotation with the arm in approximately 40 degrees abduction in the plane of the scapula and active assisted ROM in extension, horizontal adduction and internal rotation”
We spend a fair amount of time discussing this diagnosis in PT school. I wish they had just covered this type of study so that we would know the way to treat this type of patient, instead of all of the theories and possible ways to treat this patient. It is good to have understanding, but it is better to have successful outcomes.
Excerpts taken from:
Kelley MJ, Mcclure PW, Leggin BG. Frozen Shoulder: Evidence and a Proposed Model Guiding Rehabilitation. JOSPT. 2009;39(2):135-148.