“affecting 60% to 80% of individuals during their lifetime”
This statistic gets thrown around so much that all PTs should know this without thinking about it.
LBP is such a common occurrence that many non-healthcare professionals are giving advice about how to fix it.
I was at a fundraiser recently and I heard people talking about back pain as part of the conversations had between laypeople. This is how prevalent that it has become, discussions of back pain have made their way into everyday conversation. Everyone and their mother has a remedy for it.
I heard about cutting out sugars, rolling on tennis balls and soaking in Epsom salt. It wasn’t until someone in the group turned to me (they had a previous knowledge of the website) that people stopped giving advice and started asking for information.
The public wants information. On that note, if you’ve found any information from this website helpful…please share it so others can learn.
“total annual direct healthcare costs in the United States incurred by patients with LBP were estimated at $90 billion in 1998, 60% higher than individuals without LBP.”
🤔
Sounds like we can start to create a change in total costs if we could just be better at treating this issue.
Back pain is top 5 reasons a person seeks out a healthcare provider.
We are spending so much money on this problem…you’d think we’d be making a dent in the number of people with back pain, and the expenses incurred for this ailment.
Nope!
Reading the rest of this post will start to shed light on why our system, as a whole, has a lot of sucky (scientific term 👍) parts.
“Recent reports suggest that the use of physical therapy for patients with LBP is increasing.”
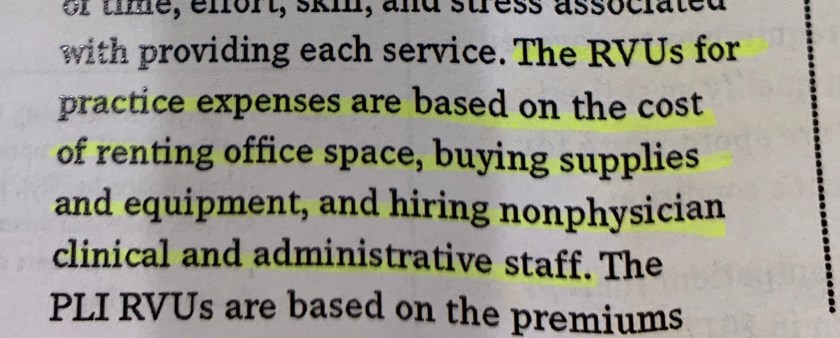
This makes so many people tho I that our profession (as a PT) is booming. Yes, there is a bigger pool of patients daily, but insurance payments have been decreasing for decades.
This is a different conversation, but it also plays a role in why clinicians may choose on intervention over another.
Soapbox
***For instance, if there are 3 people in the clinic at the same time (which could be considered fraudulent if this is occurring for patients using Medicare as insurance), the therapist has to make the patient perform some activities independently (which also should not be billed for patients with Medicare) or they would have to place the patient on a non-effective piece of equipment in order to be paid, while the PT works with another patient. ***
It then makes sense that the use of PT is increasing if we are performing ineffective techniques in order to maximize reimbursement. Not all PTs operate in this fashion, but if the above scenario sounds familiar…go get a second, third or fourth opinion.
“…Consistent in recommending an active approach to pair with emphasis on maintaining and promoting activity, while avoiding passive interventions such as bed rest or physical methods (heat/cold, ultrasound, etc.)”
Look folks, doing nothing gets you nothing. We know this in many aspects of life. Don’t work, don’t get paid. This is no different.
If the patient doesn’t play an active role in the process of rehabilitation, the results tend to be no better than doing nothing…because that’s exactly what the patient is doing in many cases.
For instance, if a patient goes to physical therapy and the patient lays there while “therapy” is performed on the patient, then the patient has little active role aside from showing up and paying.
This has become such a problem in our profession that our national organization had to come up with a short read to help patients understand what generic therapy look like during an episode of care.
“…Adherence to this recommendation for an active approach was associated with better clinical outcomes of physical therapy, with fewer visits in lower charges for care.”
If a patient learns a home program that has been shown, in the clinic, to be effective at reducing that specific patient’s complaint, why should that patient go to a physical therapy session to get unproven passive treatment or to simply repeat the same exercises over and over?
I’ll wait for your response…because I don’t know the answer to this question aside from the fact that increasing a patient’s frequency in therapy also increases the total profits of the company benefitting from the therapy.
“… it is now understood that the natural history of LBP includes subsequent periods of exacerbation and recurrence for most individuals.”
A high percentage of patients, anywhere from 25% up to 80%, experience multiple periods of low back pain during the lifespan.
How one defines recurrence has a huge role in how this number is determined. It used to be that researchers would look at a group of patients with low back pain and then see how many of them had back pain one year later. The problem with this approach is that for many of the patients, the pain never went away from the first episode.
How can this be classified as a recurrence if it never went away?!
Better questions were then asked and about 25% of patients experience at least a period of one month of relief before having a recurrence.
Because of this, it is prudent for the PT (physical therapist, not personal trainer) to teach the patient how to self-manage and to reduce as many risk factors that one particular patient has for developing back pain in the future.
“The ratio of active: passive codes had to be at least 3:1 for each phase, and every visit had to have at least one active code for the patient care to be considered inherent to guideline recommendations.”
I think that this is very conservative.
This means that for each hour a patient is seen, anywhere from 8-22 minutes are spent on manual (hands on) therapy, ultrasound, electrical stimulation, heat, ice.
The other 38-52 minutes are spent working on balance, exercise, returning to a functional activity.
This type of scenario would allow for 3 units of an active charge (75% of the session) and 1 unit of a passive charge (25% of the session).
Keep in mind, a clinician doesn’t have to follow this type of ratio, but a higher ratio of passive treatment is not consistent with the guidelines of treating patients with back pain.
“Consistent with previous studies, a successful outcome was defined as achieving at least 50% improvement on the 0SW – disability score.”
I’ve seen many patients that have gone through an episode of care without any relief before coming to see me in the clinic. For patients to get a 50% improvement in symptoms and ability to live the life they want, many would be happy with that outcome. In the research, we see as little as a 2-3 point change being considered significant when using the (pain scale). A 50% improvement is considered significant.
“471 patients with LBP met the criteria for inclusion. (18-60y, at least 3 visits of PT, duration of PT at least 10 days, initial OSW >10%, and no surgery recorded)”
This simply shows that there were a large number of patients that could be studied.
The inclusion criteria is important because it’s hard to take a study and apply it to a patient that doesn’t fit the inclusion criteria. For instance, this study included people from age 18-60. The results of the study may not apply to those under the age of 18 or over the age of 60.
Also, the study may not be applicable to those that experienced a back surgery.
“132 patients (28.0%) received adherent care and 339 (72.0%) received non-adherent care.”
Less than 1/3 received care that was consistent adherent to an active plan of care. This is disturbing!
This means that many patients going to therapy are having treatment DONE TO THEM instead of DONE WITH THEM!
There are many treatments that can be billed without the therapist directly treating the patient one-one. For instance, mechanical traction can be performed while the therapist is treating another patient. Other treatments that can be performed while the PT is treating another patient is “electrical stimulation”, moist heat and cold packs.
“Patient receiving adherent care experience greater improvement in disability, and pain intensity, and were more likely to experience a successful physical therapy outcome than patient receiving nonadherent care.”
This literally means that when patients are doing more for themselves, they get more from PT. It doesn’t have to be hard.
The PT should act as the guide in order to introduce the patient into a more pain-free, more functional and self-sustaining state. If the PT is acting as the “hero” of your story and not the “guide” in your story, it may be time to find another PT.
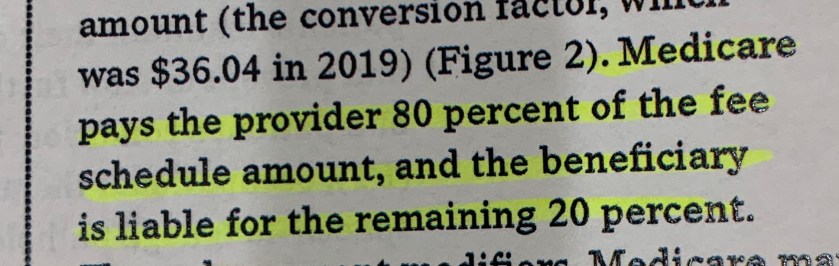
“Patient receiving adherent care also attended fewer physical therapy visits, had a shorter length of stay, and lower charges for physical therapy care.”
Fewer therapy visits = less money!
Is it getting easier to see why some clinics are more than happy to perform traction and electrical stimulation to patients?
💵💸💰
In the end, the patients are rarely at the center of care. Physical therapy is also is a business. Businesses function based on profit.
When you find a PT that treats you as a patient and not a $$$, then you have found the right person.
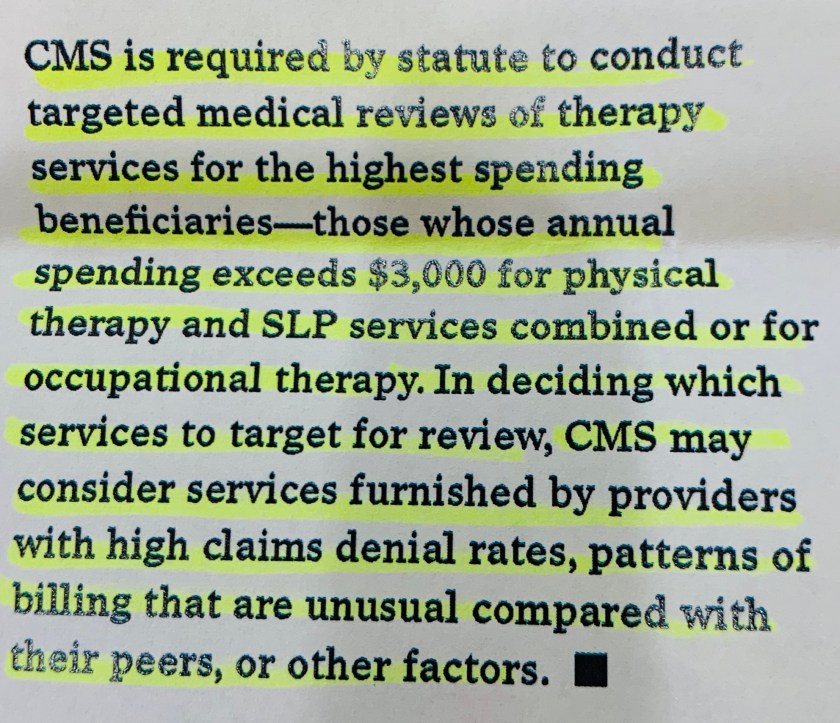
“296 patients (62.8%) had billed charges for additional healthcare related to the management of LBP in the 1-year period After completion of the physical therapy episode of care.”
It is common for patients with back pain to go to multiple providers, such as pain management, orthopedic surgeons, chiropractors and other PTs in order to seek treatment throughout the year.
“Receiving adherent care was associated with decreased use of prescription medication…also associated with a decreased likelihood of receiving diagnostic imaging procedures…associated with decrease use of MRI”
This is simply saying that when patients do more activity in physical therapy (PT), that the patient is less likely to seek out imaging.
There could be many reasons for this outside of just being active in therapy. This is purely conjecture, but if the therapist is able to educate the patient on when imaging is needed and the patient buys in, then it may have a rom in future imaging.
If the therapist demonstrates to the patient that they are strong and robust through the exercises or movements performed in therapy, then the patient may believe that the injury is less severe than initially believed.
If the therapist can change the patients belief system in order to understand that what is seen in imaging may not give them the answer they are looking for, the patient may be less likely to get imaging.
The one constant in all of this is the patient-PT relationship. It may be harder to foster that patient in an environment where multiple patients are being seen at the same time compared to when a patient is seen one-one.
These are great questions to ask when calling a PT clinic to inquire about treatment prior to actually signing up
1. How comfortable are your PTs at treating LBP
2. Do I need to use electrical stimulation and how many patients is this used on in your clinic?
3. Will the therapist be treating more than one patient at a time?
You have the right to this information prior to signing up. If you don’t care about this information, then don’t bother. If it is important to you that you have the individual attention you are paying for…ask away.
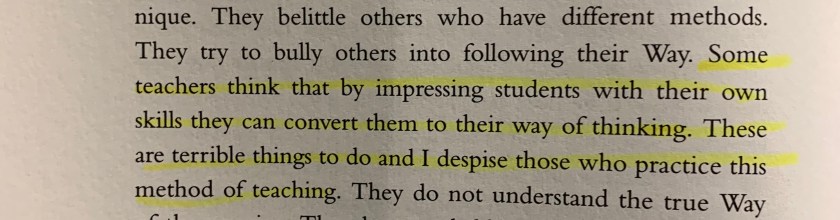
“Similar to other healthcare providers, it appears that physical therapy care for patients with LBP is characterized by widespread and unwarranted variations in practice”
We see PTs using craniosacral therapy , dry needling, MDT and other methods/interventions to treat back pain. Because of the variability, it is imperative that the PT ask about previous treatments because there is no common standard with physical therapy.
“…it may be surprising that adherence to an active approach has been reported to be low in studies of both primary care physicians and physical therapists”
Nope! ❌🙅♂️
When determining what interventions have the least amount of friction in order to get paid, the passive interventions win every time.
It’s unfortunate, but until insurance based physical therapy is linked to total costs for the treatment issued to a patient (such as a large lump sum issued to the clinic at the beginning of the year in order to manage a patients physical therapy needs and complaints), we will continue to see passive treatments as they reimburse with little time spent with patients.
Excerpts from:
Fritz JM, Cleland JA, Speckman M et al. Physical Therapy for Acute Low Back Pain: Associations with Subsequent Healthcare Costs. Spine. 2008;33:1800-1805.