
 You are not your MRI…at least not for long.
You are not your MRI…at least not for long.
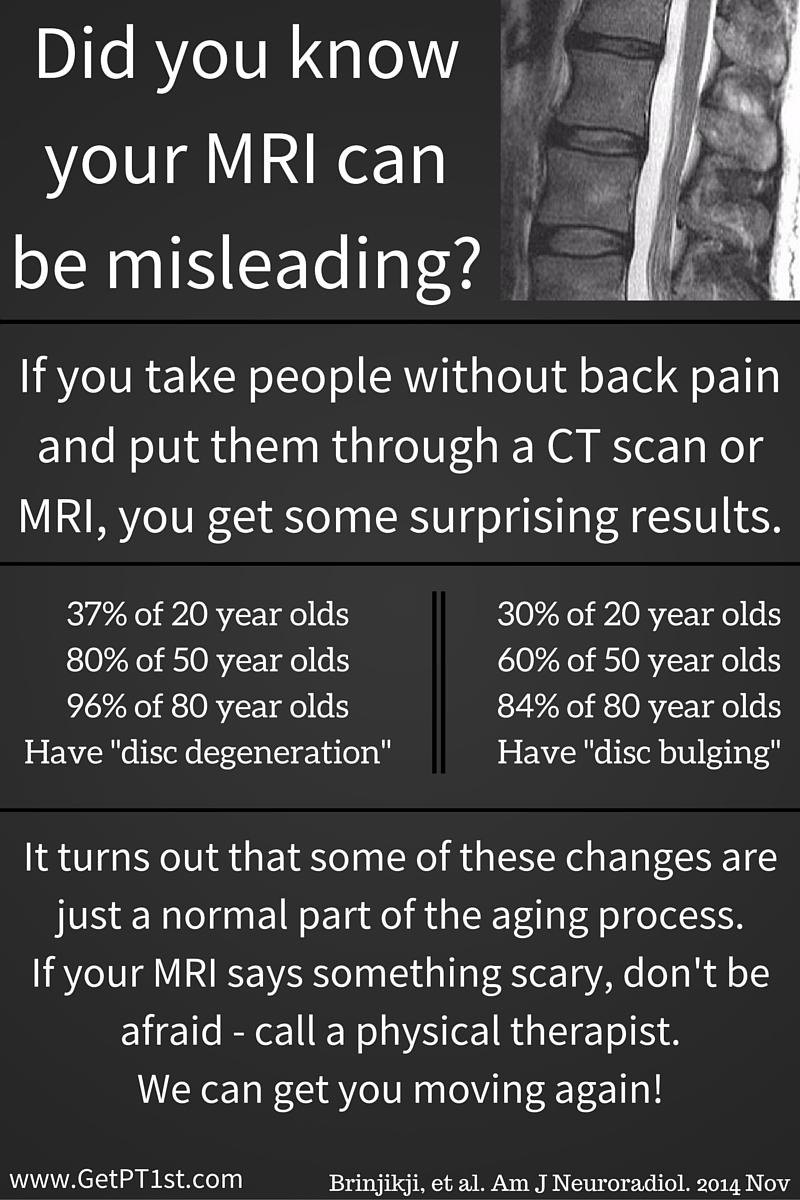
MORAL OF THE STORY: Stop your whining over your herniated disc, bulging disc or exploding disc. You are probably not the outlier. If your pain is lasting longer than six months, your disc is probably healed, but you still move like crap. Start to move better and take better care of yourself and the improvements will follow. In general, this means that you are most likely the problem…not your back.
Also, I will be taking a couple of weeks off from reading and writing to travel with the family. Taking some time to breathe. If you enjoy the blog, please add a topic that you would like to see covered at a later date.
- “Lumbar disc hernia (LDH) is a common cause of low back pain and radicular leg pain…majority of LDH patients recover spontaneously…Purpose of the present study was to investigate the natural history of the morphologic changes of LDH on MRI and to assess correlations with the type of LDH and the clinical outcome”
First, disc herniations are a common cause of pain. I believe this to be true and the research consistently reports this fact. The part that doesn’t get reported is the second part of the statement being that spontaneous recovery is normal.
When people come into the clinic, they have this seemingly rehearsed story of how they had an MRI and was told that they have a bulging/herniated/exploding (maybe a little overboard) disc. The doctors never tell them that this can recover on its own and patients then wear the herniated disc patch for the rest of their lives.
As you will see, you no longer need to wear that patch if your were told that you have an exploding disc.
- “…42 patients…mean age of 42…unilateral leg pain and low back pain…symptomatic level was L2-3 in 8 cases, L3-4 in 6 cases, L4-5 in 15 cases and L5-S1 in 13 cases”
Let’s start here. 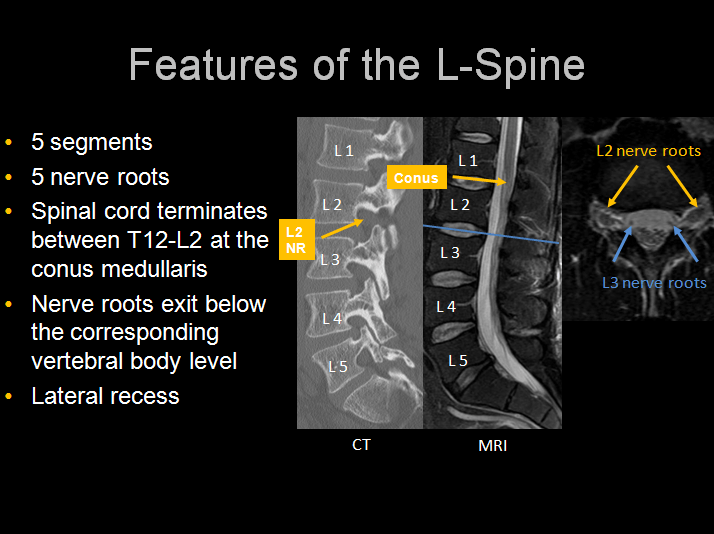
The lumbar spine is labeled as L1-5 and the sacral spine then starts. The intersection between the lumbar spine and the sacrum is L5-S1. The segments are named by the upper segment first-lower segment second.
Some interesting notes regarding this study:
- 66% of the patients have symptoms coming from the lower lumbar segments, those being L4-S1. This is inconsistent with published research reporting that up to 95% of symptoms come from these lower segments.
- Therefore, 34% of symptoms are coming from the upper segments. Again, previous research notes that only 5% of symptoms come from these segments.
Unilateral leg pain simply means that only one leg is affected. For those that may have experienced sciatica in the past, you will remember that it was only one leg that experienced symptoms. If you have symptoms in both legs, then it may not be sciatica.
- “All patients underwent MRI examinations every three months for a period of 3-24 months”
This is not affordable for most and won’t be approved by any insurance that I have encountered. The reason for the frequent MRI’s is to see how things change over time.
- “LDH was classified into three types: protrusion (n=7), extrusion (n=17 and sequestration (n=18)”
Here comes the jelly donut theory. If you have heard it, then you can pass this paragraph up. Think of the disc as a jelly donut (I know that this is an oversimplification, but this model makes the most sense…even if it is not the most accurate).
A protrusion means that the outer portion of the donut (the actual donut itself) has been deformed. If you plug the hole of the jelly donut so that the jelly can’t come out of the hole, you will be able to follow along with the rest of the idea. I personally don’t like jelly donuts. I much prefer custard or cream. Speaking of that, Tim Hortons has the best filled donuts that I have ever had. This reminds me of a trip to Canada with my best buddy Carl. If I have the time later, some stories from this road trip may come out. Back to business; if you squeeze the donut on an edge lightly, you will start to squeeze the jelly away from the area that you are squeezing. If you squeeze a little harder, you will see the donut “bulge” just prior to the jelly coming out. This is a protrusion.
An extrusion means that the jelly has escaped! Oh no! Now what? No big deal. You will see later that this may actually be a better situation for you than the protrusion.
A sequestration means that not only has the jelly escaped, but a piece has broken off and hit the floor. If enough nuclear material (the jelly inside the disc) breaks through the annulus (the donut in the example), then it may break off and be free floating in the spinal canal (near the nerves of the spine). This again may not be as bad as it sounds.
- Correlation between the clinical outcome and spontaneous changes of the herniated mass on MRI (6 months)
| MRI change | Excellent | Good | Poor | Total% |
| Disappearance | 6 | 2 | 0 | 19 |
| More than 50% reduction | 11 | 18 | 0 | 69 |
| Little or no reduction | 0 | 1 | 4 | 12 |
| Total | 40 | 50 | 10 | 100 |
What this means is that in 19% of patients, the herniation seen on the MRI disappeared over the course of time. Better yet, about 88% improved significantly over the course of time. You are not your MRI… at least not for long.
6.
| Type of herniation | Case | Duration of symptoms |
| Protrusion | 3 cases in total | 3-14 weeks with 8 weeks average |
| Extrusion | 17 cases | 4-8 weeks with 4.8 weeks average |
| Sequestration | 18 cases | 1-5 weeks with 3.2 weeks average |
What does this chart mean? Those that have a “more serious” appearing herniation on MRI actually respond faster than those with a smaller herniation. You are not your MRI…at least not for long
Excerpts taken from:
Takada E, Takahashi M. Natural history of lumbar disc hernia with radicular leg pain: Spontaneous MRI changes of the herniated mass and correlation with clinical outcome. Journal of Orthopaedic Surgery. 2001;9(1):1-7.
 SCIATICA OF THE ARM
SCIATICA OF THE ARM
{kind=link}